All published articles of this journal are available on ScienceDirect.

Preliminary Testing of Efficacy of the Invented Sensory Re-education Device (SRED) on Patients with Peripheral Neuropathy
Authors Info & Affiliations
Abstract
Background:
Sensory rehabilitation is considered one of the challenges and a persistent functional deficit in the long term. All rehabilitation paradigms use re-education in many different ways. The main issue here is that the brain mostly recognizes, considers and reacts with structured, and consistent input. Likewise, all the sensory rehabilitation techniques try to use a systematic input (type, pattern, timing and intensity) to regain or re-establish any type of sensation but none of these are perfectly systematic.
Methods:
For this reason, we developed a Sensory Re-Education Device (SRED) which allows a systematic sensory input “type, pattern, timing and intensity input” supported by software to operate the system and manage the data. Five senses (light touch, pinprick, hot-cold, vibration, and smell) were uploaded and constructed to allow different types, intensities, frequencies, patterns, and timing. Eight cases of Breast Cancer (BC) post-chemotherapy and Diabetes Mellitus II (DM2) were recruited for eight sessions. (Only hot-cold, smell, and light touch were used in this trial.)
Result:
The outcome was very impressive, as most of the patients regained their sensibility at a rate of over 80%.
Conclusion:
The outcome and the related treatment factors were showing a positive consistency. This is very encouraging, though a large sample is required to establish significance. The team members welcome any feedback, suggestions, and critiques via the PI email below.
1. INTRODUCTION
Sensory re-education is a therapeutic rehabilitation program that uses repeated sensory stimulation to help sensory-impaired patients recover functional sensibility in the affected area and learn adaptive functioning [1]. Many approaches toward sensory stimulation are employed to provide input to sensory receptors and pathways. Several forms of stimulation may be used, including electrical stimulation, skin stroking with textured, friction-producing items such as Velcro; and the use of specially modified instruments and tools [2]. Other procedures and modalities that may be used include muscle and joint actions, vibration, pressure, biofeedback, various forms of movement, and tactile stimulation [3]. There are other sensory activities that require attention to the senses and cognitive actions. Sensory re-education may be provided in indirect ways as part of a larger set of therapeutic techniques rather than as an independent, distinct treatment [4].
Among the goals of sensory re-education, one is to retrain neural pathways and responses to stimuli in order to restore patient's sensory perception [5]. Increased sensory input and activity may help to stimulate nerve regeneration and growth. In addition, previously unused neural connections may be trained to take over for damaged pathways. This neural plasticity can be used to the advantage of a patient with nerve damage or impairment.
Some scientists believe it may be possible for remapping to occur in the brain, so that connections between areas of the brain and certain parts of the body, as represented on Penfield maps, can adapt and change after nerve injury or amputation [1, 6, 7] thereby causing new connections that relay sensation. However, the Central, Nervous System CNS has its gaining and learning characteristics that control, arrange Ingram, code, and save. The most agreeable method is through simple sequential intensive, graded, and repeated patterns. Progress should be gradual and achieved through the use of accompanied patterns that are tightly organized in a consistent and structured mode [8].
Sensation has evolved to make use of the brain’s hierarchical structure. All concepts are built from smaller concepts, all the way down to the most fundamental thoughts. This array of recursively linked concepts is called “conceptual hierarchy” [9]. Likewise all sensory rehabilitation techniques must use the systematic input (type, pattern, timing, frequency, and intensity) to regain or re-establish any type of sensation [10, 11]. Therefore, it is necessary to employ a structured systematic approach toward sensory rehabilitation. To that end, the aim of this project is to design a Re-Education Sensory Device that delivers, records, and stores systematic sensory stimulation data that helps diagnose and treat patients with a sensory deficit. The golden concept of this system is the capacity to deliver a systematic (consistent, regular, specific, pattern, timely, and controlled intensity) input that enables the brain to code and Ingram the function and recognize the physical properties of frequency and wavelength.
2. METHODOLOGY
2.1. SRED Components and Concept
The multi-sensory stimulation approach through the use of a Sensory Re-Education Device (SRED) is a therapeutic program that employs sensory stimulation to help with the functional recovery of sensory loss and to help patients learn adaptive functioning. It assists patients with various forms of sensory loss and impairment in retraining their sensory pathways, adapting to their changed abilities, and regaining sensory function. The SRED achieves the main goal of re-education by delivering a systematic (consistent, regular, specific, repeated pattern, time, and intensity control) input that enables the brain to code and Ingram the function and recognize the physical properties of frequency and wavelength.
The SRED is designed to be flexible and easy to operate so that the patient can develop skills/abilities, mental experience, and function recognition through continuous and intensive training.
Earlier studies have indicated that successful training may change the way in which the brain controls movement and have demonstrated remapping of movement representations in the primary motor cortex after effective rehabilitative training of sensory impairments8. To date, no SRED has been developed, tested, and approved for re-educating the re-educating subjects with a sensory deficit.
The sensory system has a great capacity to act and interact with the surrounding environment. The SRED stimulates multiple senses through the use of different programs. Continuous and repeated sensory stimulation helps patients with Chemotherapy-induced peripheral neuropathy CIPN and enables the occupational/physical therapist to work on impaired sensory areas and to mend damaged cells. Hence, the present study was planned to assess the efficacy of the SRED developed to provide sensory re-education of subjects with CIPN.
This is the first prototype that has been developed based on the results attained by its predecessor machine. The device has two driving parts, which contain hardware and software.
2.2. HARDWARE
2.3. Software
The software is built on Visual Basic with MS Access Database. It interacts with the hardware through a communication port called Com.Port, which is connected via USB to Arduino Mega. In Visual Basic, we use a Windows HyperTerminal communication module to interact with the hardware. Following are the major modules in the software.
Add Patient: This is a patient-adding module in which we record new patients or modify existing ones.
Session Module: This is the main module in which we test the patient’s senses. It is the most complicated module in the software. In this module, we use external hardware (Fig. 1) and get values to generate results. There are two types of results marked: One is automatic, which is generated by the system according to the input and output from the patient. The other is manual, which is controlled by the doctor (operator). Automatic results are based on full statistics that are generated by the calculation of the input dose, output result, and time is taken to obtain an answer. The total and maximum values for each question (acquire) in the system are set beforehand so the system can calculate the results based on answers given by the patients, automatically dividing them with the maximum value which has already been given.
Reporting Module: The module is where we analyze patient’s improvement and session details based on the time taken to answer various questions. We conduct an overall evaluation and find the weakest senses in which to make improvements. Variables related to frequency, intensity, timing, etc. were taken into account. The storing, tracking, and recalling of data were handled very well.
2.4. Building the Device
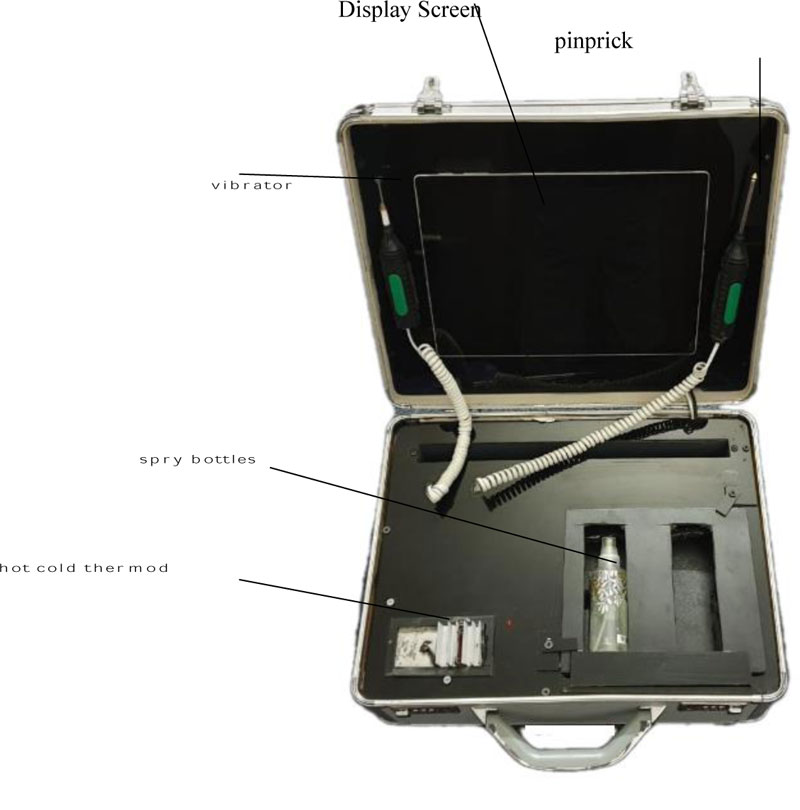
After testing the prototype device, we began creating the final compact shape. We fitted it in a small 50cm*40cm*20cm metal briefcase. This portable size makes the system appropriate for hospitals, clinics, and home use. All accessories were mounted in the briefcase. We used an acrylic sheet incubate hardware, which we had to install in the device.
At the top, we created a fitting to hold the display, vibration device, and pain prick device. At the bottom, we affixed circuits and other accessories used in the device. Before fixing, we cut an acrylic sheet that would cover the entire base to make fittings for the keyboard, spray bottles (Fig. 2), hot and cold Peltier. Beneath it, all the circuits and modules were installed.
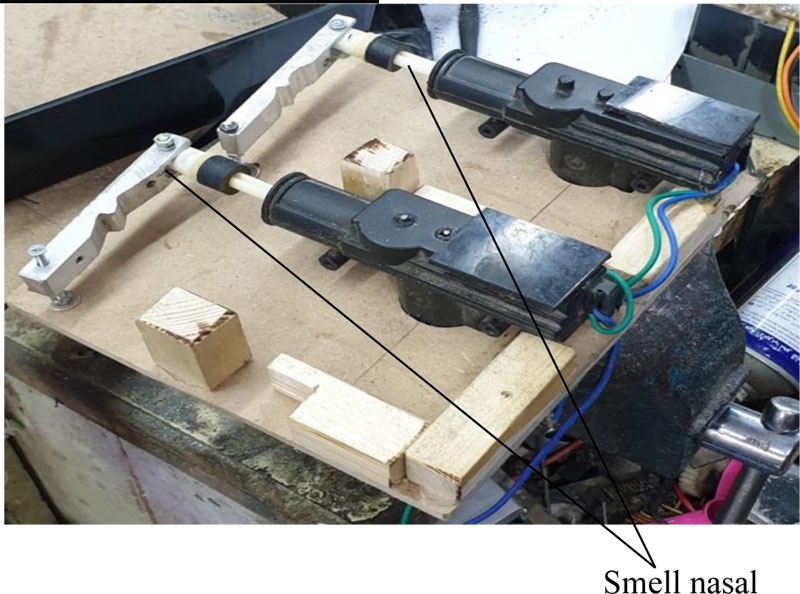
The spraying mechanism consists of a servo motor, un-load circuit.
The drive circuit delivers 5VDC to the relay to make contact for the delivery of 12VDC to the servo motor for one second, to exert the required force on the spray nozzle. The entire mechanism is very simple, durable, and convenient to operate and use. The relay takes commands from the drive circuit which is Arduino Mega. Both sprays share an individual drive relay circuit to function.
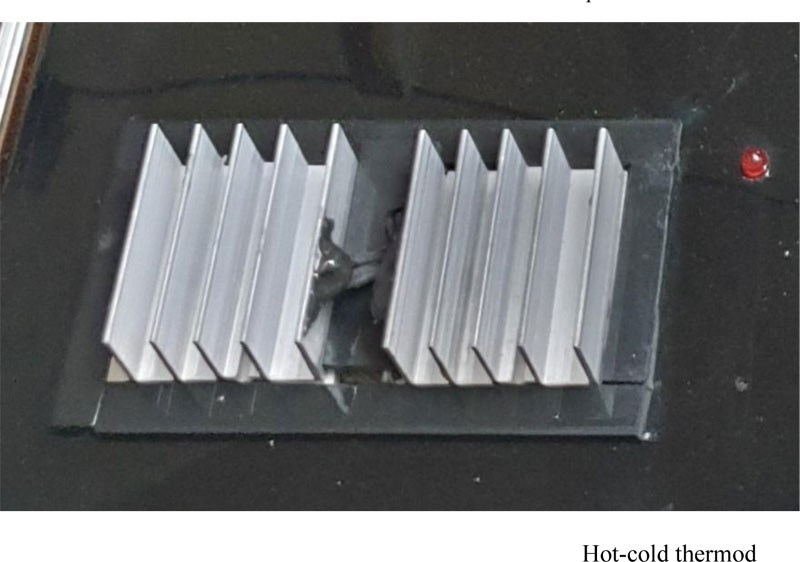
Hot-cold thermod
Two individual peltries are installed to generate hot and cold temperatures. The peltries are installed on a heartsick alloy to produce controlled temperatures. The peltries are derived from the relay module, which takes commands from the microprocessor. In addition, two temperature sensors are installed to provide the current temperature.
All the circuits and modules are placed underneath the bottom section. AC220 power goes to the power supply for peltries while a 5VDC power module powers the relay modules and Arduino. The display adapter is also placed in the same section.
2.5. Study Design
This study is a quasi-experimental one-group pre-post study. Participants will be studied before and after the device is used as an intervention. During the first session, baseline outcome values will be compared to the same outcome values at the end of the last session (session 5) to evaluate the efficacy of this device in improving CIPN associated with chemotherapy and DM peripheral neuropathy. The mechanism, cause, and pathology of the neuropathy are beyond the scope of this study.
2.6. Study Population
The study population consists of patients with peripheral sensory loss due to chemotherapy treatment of breast cancer (BC) and patients with peripheral sensory loss secondary to DM. While this paper addresses a pilot sample, full details will be published upon completion. The study investigated smell, hot-cold, and light touch sensations. The study is conducted in regular physiotherapy, occupation therapy department of KAMC, NGHA, Riyadh.
The subjects included in the study were selected based on the following inclusion and exclusion criteria. Inclusion: Adult DM and BC patients in the age group of 18-60 years. Breast cancer patients who underwent chemotherapy or radiation therapy and chronic DM with a confirmed diagnosis of peripheral neuropathy. Exclusion: Patients <18 years old or >60 years old, patients on palliative care, patients with degenerative neuropathy or acute inflammation, patients with an implanted device and who are not willing to provide informed consent were excluded from the study. Each patient was required to sign a consent form after the study’s details were explained and all questions about the experiment were addressed.
Patients were invited to a (day-care) program to facilitate the conducting of long, repeated sessions throughout the day.(Fig. 4) The smells of various perfumes were delivered in different concentrations via nasal spray at a graded distance. Concentration and distance were modulated in certain paradigms at a small cabinet to maintain the concentration of the smell. The cabinet fan then switched on to evacuate the smell. Hot-cold (Fig. 3) air was delivered through the thermod in a graded range of temperatures. Several types of touch (very rough to smooth material) were used to re-educate the touch. All were recorded in a bulletin system, as well as in written feedback from the patient.

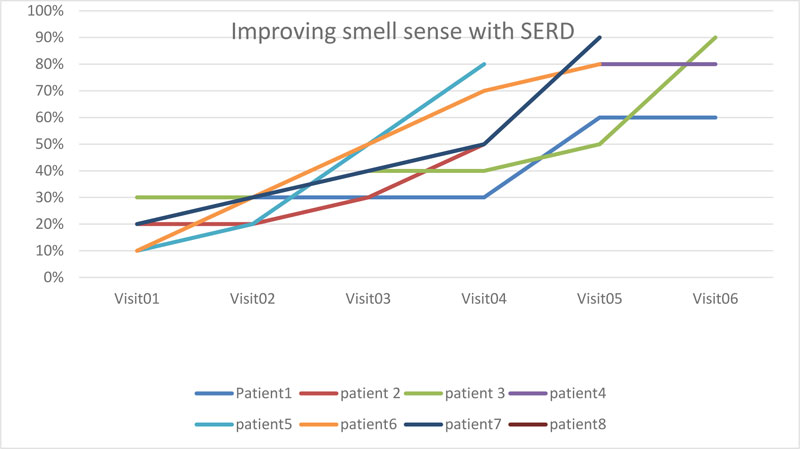
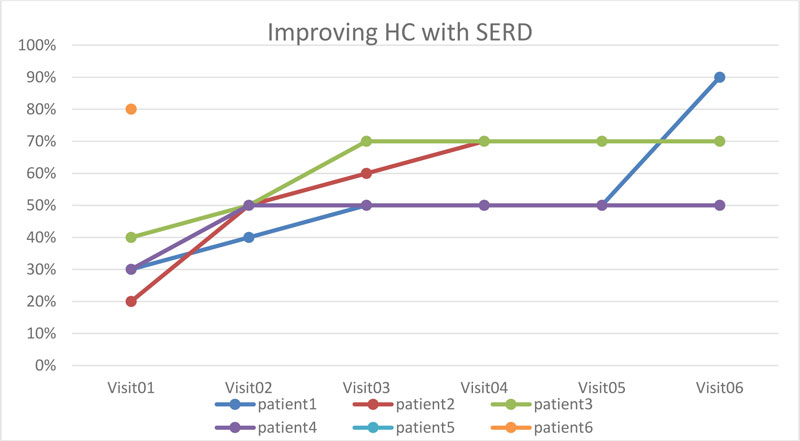
3. RESULTS
The overall trend among patients in terms of the three senses was progressive and aligned with the clinical recovery. Because the population is very small, we cannot draw a comprehensive analysis. There is a slight inclination of the progress of a few patients at the beginning, but this must be carefully observed. The trend is encouraging enough to proceed with the experiment.

4. DISCUSSION
There are real challenges involved in sensory rehabilitation, with many techniques and procedures being used to facilitate recovery. In most cases, recovery goals, rates, and efficiency were not achieved or were extremely difficult to achieve. Consistency is another challenge. With this device, the results indicated that the three sensations showed remarkable improvement. Patients’ reported feedback aligns with the outcome reported by the machine. However, the clinical comparison seems to be in favor of this system outcome. There is a lack of the outcome of conventional sensory rehabilitation
The factor being assessed here is the efficacy of the SRES (Figs. 5-7), in particular, the outcomes related to time and efficiency of recovery. This trial is intended to ensure that the system performs its tasks as required and that the software easily and smoothly manages all functions. It may be worth mentioning here that the recovery rate is not responding from the first instance; it took several tries before we achieved a remarkable note of recovery, particularly in terms of smell. Another item worth mentioning is the patient’s commitment to using this device. Patient feedback aligns with the outcome reported by the machine.
CONCLUSION
A postive trend of recovery was noted all the way; many cases need to be recruited. The remaining sensory modalities will be included. The whole work will be published and a full date will be presented including the builtin data in a very comprehensive article.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The research has been approved by the King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudia Arabia with approval number RC17\323\R .
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from each participant prior to the study.
STANDEREDS OF REPORTING
CONSORT guidelines and methodology has been followed.
FUNDING
This study has been funded by the King Abdullah International Medical Research Center (KAIMRC).
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

