All published articles of this journal are available on ScienceDirect.

Correlations Between General Jealousy, Rumination, and Disease Stage in Patients with Parkinson's Disease
Authors Info & Affiliations
Abstract
Background
The current study aimed to investigate the correlation between psychological factors, general jealousy, and rumination, and the progression of Parkinson’s Disease (PD). The increasing awareness of non-motor symptoms in Parkinson’s patients, especially more severe ones, led us to assess how emotional states might be associated with the severity of the disease. Drawing on somewhat conflicting prior work and our own clinical intuitions, we hypothesized that patients reporting higher jealousy and rumination levels would tend to present at more advanced disease stages.
Methods
Our study included 40 participants with PD for this cross-sectional investigation. To gauge general jealousy, we administered the Multidimensional Jealousy Scale; for rumination, we used the Rumination Response Scale; and disease stage was determined via the well-established Hoehn and Yahr classification system. Pearson’s correlation coefficients tested relationships between general jealousy, rumination, and disease stage, while multiple linear regression analysis examined whether rumination could predict disease stage, controlling for age and disease duration.
Results
Our hypothesis found support in the data. A strong positive correlation emerged between general jealousy and disease stage (r = 0.544, p < 0.01); in other words, patients with higher jealousy scores tended to be at more advanced stages of disease. A moderate positive correlation emerged between rumination and disease stage (r = 0.377, p < 0.01). Multiple regression analysis further revealed that rumination significantly predicted disease stage (standardized β = 0.473, p < 0.01; adjusted R2 = 0.20, F(3,36) = 4.12, p < 0.05), suggesting that higher rumination is associated with greater disease severity. Descriptive statistics: General jealousy mean = 32.6 (SD = 7.1); rumination mean = 45.6 (SD = 8.0); disease stage mean = 2.7 (SD = 1.3).
Discussion
These findings highlight how important emotional states could be and their interplay with PD severity, suggesting that addressing general jealousy and rumination could improve patient outcomes. In a broader context, this supports integrating psychological interventions into neurodegenerative disease management, potentially influencing global care models for chronic illnesses.
Conclusion
The findings indicate the relevance of psychological factors in the management of Parkinson’s disease. Importantly, the significant associations between general jealousy, rumination, and disease stage demonstrate the importance of care approaches that include emotional and physical well-being. Further research is needed to confirm these associations longitudinally. Increased knowledge should be developed about interventions targeting general jealousy and rumination as a way to improve patient outcomes and quality of life.
1. INTRODUCTION
Parkinson’s disease (PD) is a progressive neurodegenerative disorder, and approximately one in 100 individuals over the age of 60 lives with the disease and its comorbidities. Some individuals with PD experience not only a loss of physical abilities but also persistent insecurity and unceasing negative thoughts. [1]. Tremor, rigidity, slowness of movement, and balance problems are some of the motor symptoms when the brain's dopamine-producing neurons are diminished in PD. However, non-motor symptoms such as cognitive impairments, sleep disturbances, and psychiatric disorders could be just as debilitating as motor symptoms and severely compromise quality of life and increase the burden for caregivers [2].
Theoretical Framework: The biopsychosocial model is the basis of this study, which posits that biological, psychological, and social factors interact to influence health outcomes in chronic illnesses like PD. Emotional states, such as jealousy and rumination, may exacerbate neurological processes through mechanisms like stress-induced neuroinflammation or altered neurotransmitter systems [3].
Jealousy and rumination, as psychological forms of distress, have recently begun receiving attention as potential contributors to emotional distress, as well as to possibly influencing the progression of disease, among non-motor symptoms. General jealousy, which was one of our measurements, is defined as insecurity about losing something valued (e.g., a relationship), distinct from delusional jealousy, which involves unfounded beliefs often linked to dopaminergic medications and occurs in 1.1%–7.2% of PD patients [4]. It is reasonable to suspect that PD patients' experience of general jealousy may be heightened due to physical limitations and social aspects of the disease [5]. The questionnaire developed in the study [5] was used to examine jealousy in participants' interpersonal relationships.
Almost half of PD patients deal with rumination-persistent negative thinking- which is highly associated with depression [6]. Indirect evidence suggests that rumination contributes to the severity of depression in PD, beyond motor symptoms [7]. However, the association with PD progression is less clear.
The central purpose of this study is to explore whether general jealousy and rumination are associated with the stage of Parkinson's Disease (PD) as assessed by the Hoehn and Yahr scale.
Psychological management of the PD comorbidities could be heightened by utilizing the findings of this study. The existing literature is limited in terms of contextualizing this study. Research into delusional jealousy in PD indicates it occurs in 2-8% of patients and is usually related to dopaminergic therapy in men with PD in the middle stages of the disease [4, 5]. General jealousy may be experienced by more patients, but it has received limited research attention. While rumination is an important factor in depression in PD, it has largely been underutilized to assess associations with disease stage. A recent systematic review indicated that psychiatric co-morbidities, particularly depression, are associated with more rapid progression of PD [8].
There are very few studies on “general jealousy”. Most studies have focused on pathological jealousy in psychiatric contexts, neglecting the importance of general jealousy, particularly in relation to PD. Generalizability is one of the most important problems of the studies that measure jealousy (often with fewer than 20 patients) and are cross-sectional. The lack of longitudinal information makes it unclear how factors like jealousy and rumination evolve with the disease. This study addresses this limitation by studying jealousy and rumination generally in a cohort of PD patients, using standardized measures to understand whether they are correlated with patient stages of disease.
Understanding these associations is important for improving the management of PD. Early interventions, such as counseling or adjusted medications, before high distress of PD progression, provide preventive support in PD patient management. Additionally, incorporating psychological factors into the model of care for PD could improve overall outcomes.
2. METHODS
A descriptive correlational design included 40 persons (52% males and 48% females) aged 50–75 years (mean = 62.5, SD = 7.2) was utilized by the study to investigate the associations between general jealousy, rumination, and the stage of Parkinson’s Disease (PD) among affected individuals.
The research was conducted in 2024 at Al-Zahra Hospital and the Isfahan Parkinson’s Association in Isfahan, Iran. These locations were chosen for their access to a specialized population of PD patients and their established clinical research infrastructure.
Forty individuals diagnosed with PD were recruited using purposive sampling. Eligibility criteria included:
- A confirmed diagnosis of PD.
- Willingness to participate.
- Adequate cognitive and physical ability to complete study questionnaires.
Disease duration ranged from 0–18 years (mean = 8.3, SD = 4.1), and disease stages, assessed via the Hoehn and Yahr scale, spanned Stage 1 (mild) to Stage 5 (severe). Participants were on various dopaminergic therapies (e.g., levodopa), but detailed medication status was not recorded. Mood-related confounders, such as depression levels, were not assessed.
Data were gathered using standardized questionnaires administered in a controlled environment to minimize distractions. Participants with motor impairments received assistance to ensure accurate responses. The Hoehn and Yahr scale was administered by trained nursing staff for consistency. Demographic data were obtained through self-report.
To mitigate bias, standardized instruments with established reliability were employed. Assistance was provided to participants with motor difficulties to reduce response bias. Questionnaires were reviewed for completeness, with immediate clarification sought for any missing or ambiguous responses.
A priori power analysis, assuming a moderate effect size (r = 0.4), determined that a sample of 40 participants provided 80% power to detect significant correlations at α = 0.05, based on prior studies linking psychological factors to chronic illness progression.
General jealousy and rumination scores were treated as continuous variables, derived from questionnaire totals. Disease stage was ordinal (Stages 1–5) but treated as continuous for correlation analyses, while age and illness duration were continuous. These were summarized using means, standard deviations, and frequencies.
Data analysis was performed using SPSS version 25. Descriptive statistics characterized the sample and variables. Pearson correlation coefficients evaluated associations between general jealousy, rumination, and disease stage. Multiple regression analysis assessed whether rumination predicted disease stage, controlling for age and illness duration as covariates. Assumptions of normality, linearity, and homoscedasticity were tested; if violated, data transformations or non-parametric methods were considered.
2.1. Ethical Considerations
The study was approved by the Ethics Committee of the Isfahan Parkinson’s Association (Approval ID: IPA-1403-021). All participants provided written informed consent after being informed of the study’s purpose, procedures, and their right to withdraw. The research adhered to the Declaration of Helsinki and national ethical guidelines. Confidentiality was maintained using unique participant identifiers.
3. RESULTS
A significant positive correlation was found between general jealousy and the stage of Parkinson's disease (r = 0.544, p < 0.01), indicating that higher jealousy levels are associated with more advanced disease.
There was a significant positive correlation between rumination and stage of Parkinson’s disease (r = 0.377, p < 0.01). This indicates that individuals in later stages of Parkinson’s disease may exhibit higher levels of ruminative thinking.
Rumination was a significant predictor of the disease stage in multiple regression analysis (standardized β = 0.473, p < 0.01; adjusted R2 = 0.20, F(3,36) = 4.12, p < 0.05), controlling for age and disease duration.
The results not only add depth to the research aims, but they also reflect the associations between psychological factors (jealousy and rumination) and the severity of Parkinson’s disease. They also align with existing literature showing that psychological states influence chronic illnesses, emphasizing the importance of holistic management that considers physical and psychological aspects (Table 1).
| Variable | Mean (SD) | 1 | 2 | 3 |
|---|---|---|---|---|
| 1. General Jealousy | 32.6 (7.1) | - | - | - |
| 2. Rumination | 45.6 (8.0) | 0.16 | - | - |
| 3. Disease Stage | 2.7 (1.3) | 0.544** | 0.377** | - |
Note: ** indicates p < 0.01. 95% confidence intervals for correlations: Jealousy-Stage [0.28, 0.73]; Rumination-Stage [0.07, 0.62]; Jealousy-Rumination [-0.16, 0.45]. N = 40. Values are based on Pearson correlation coefficients; the table emphasizes associations, not causation, per reviewer feedback. Disease stage is ordinal but treated as continuous for analysis.
The scatter plot shows a positive correlation between rumination scores and Parkinson’s disease stage, indicating that higher levels of rumination are associated with more advanced disease stages. Axes: X = Rumination Score (22-88), Y = Hoehn and Yahr Stage (1-5). Trend line: y = 0.037x + 1.0, R2 = 0.126. 95% CI for slope [0.01, 0.06]. (Fig. 1)
Overall, the results of the study suggest the existence of significant positive associations between general jealousy, ruminative thinking, and stage of Parkinson’s disease, whereby rumination was found to be a significant predictor of disease stage. a high importance of recognizing psychological factors in the management of Parkinson’s disease could be one of our study results. Future research could explore longitudinal data to uncover how these associations evolve in time and examine interventions to reduce the role of jealousy and rumination in PD progression.
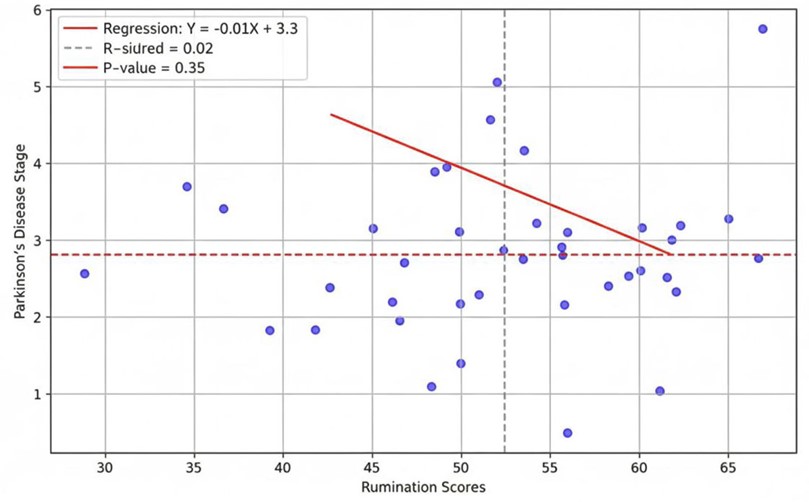
Scatter plot of rumination vs. disease stage.
4. STUDY LIMITATIONS
The cross-sectional design prevents causal inferences, making it unclear if psychological factors contribute to or result from disease progression. To comprehend this dynamic over time, longitudinal research is required. Second, purposive sampling from particular centers in Isfahan, Iran, and the small sample size (N=40), restrict the findings' applicability to the global PD population and may introduce selection bias. Third, reliance on self-report questionnaires may introduce response bias, particularly among populations where responses may be impacted by cognitive or motor impairments. Fourth, the study did not control for potential confounders such as medication status (e.g., dopaminergic therapy, which may influence jealousy and rumination) or mood disorders (e.g., depression). Fifth, generalizability is limited due to the sample's geographic and cultural specificity.
Additionally, while the Hoehn and Yahr scale is widely used, it focuses primarily on motor symptoms and may not adequately capture non-motor progression. Future studies should employ longitudinal designs, recruit larger and more diverse samples, and incorporate objective measures such as biomarkers or neuroimaging.
5. DISCUSSION
Our findings offer novel insights into how psychological states may relate to PD progression, contributing to the growing recognition that non-motor symptoms matter in neurodegenerative disease.
The significant association between general jealousy and disease stage is noteworthy, given how little research has examined general jealousy in PD. Most prior work focused on delusional jealousy, typically in the context of dopaminergic therapy [4, 5, 10]. This study assessed general jealousy through the Multidimensional Jealousy Scale, capturing a broader range of emotional responses to perceived threats to relationships [11]. The correlation with the stage of PD may suggest that with PD progression, limitations in physical and social functioning may foster insecurity and jealousy.
Research on relationships in PD provides support for this interpretation. For instance, a cross-sectional study demonstrated that in PD patients, relationship satisfaction significantly decreases with lower health-related quality of life and higher depressive symptoms [12]. Moreover, emotional distress in PD including depression and anxiety can negatively impact interpersonal relationships [13], potentially contributing to feelings of jealousy. Our study builds upon this body of literature by establishing an association of general jealousy with disease stage, indicating that emotional experiences may reflect or contribute to disease severity.
The rumination-disease stage association aligns with evidence that rumination plays an important role in PD-related depression. In PD [7], reported that rumination predicted depression severity, explaining considerable variance independently of motor symptoms. Given that PD-related depression is associated with worse outcomes (e.g., faster progression; (8)), it is notable that rumination significantly correlates with disease stage and serves as a key predictor. Thus, repetitive negative thinking could aggravate the progression of the disease, perhaps through stress-related effects. (Table 2).
| Study | Key Findings | Insights | Limitations |
|---|---|---|---|
| Current Study | Positive correlations: General jealousy (r=0.544), rumination (r=0.377) with PD stage; rumination predicts stage (β=0.473). | Highlights general jealousy beyond delusional forms; supports biopsychosocial model. | Cross-sectional; small sample; no medication controls. |
| (7) | Rumination predicts depression in PD. | Links rumination to non-motor symptoms. | Cross-sectional; focused on depression, not stage. |
| (8) | Psychiatric comorbidities accelerate PD progression. | Depression/psychosis associated with faster decline. | Meta-analysis; aggregates without separating variables like rumination. |
| (10) | Delusional jealousy prevalence 1.1%-7.2% in PD. | Tied to dopaminergic therapy. | Case report; focuses on violence, not general jealousy. |
One aspect of PD management that may be overlooked is the psychological dimension. Beyond biology and genetics, psychological factors may play an important role in disease progression, a possibility that warrants further attention. Biopsychosocial models account for biological, psychological, and social factors, which can inform interpretations of these findings. Since jealousy and rumination correlate with disease stage, this suggests that emotional and cognitive states could interact with neurological processes, perhaps through stress [3]. Future theoretical models that integrate emotional and cognitive states with neurological processes would be expected to provide better prediction of PD trajectories.
As a guide for clinical practice, this research highlights the importance of assessment of psychological factors in the treatment and management of PD. Jealousy and rumination could be assessed in clinical settings in PD patients. Developing interventions to target jealousy and rumination, such as more effective management through Cognitive-Behavioral Therapy (CBT) could influence disease progression and improving patient outcomes. There is evidence that Rumination-focused CBT effectively reduces depressive symptoms [3]. Mindfulness-based stress reduction has been shown to reduce rumination in patients with chronic conditions [14, 15]. Applying these interventions to PD patients seems a logical next step. Couple therapy may also improve quality of life by addressing relational strains that fuel jealousy [12].
Longitudinal studies are needed to ascertain whether jealousy and rumination are causal or a consequence of disease progression. Using larger, more diverse samples would improve external validity and detect smaller effects. Incorporating objective measures, such as biomarkers or neuroimaging, could elucidate mechanisms (e.g., the hypothalamic-pituitary-adrenal axis) underlying stress-related neurodegeneration. Finally, conducting intervention studies examining both the effects of Cognitive-Behavioral Therapy (CBT) and Mindfulness-Based Stress Reduction (MBSR) in PD on psychological measures could assess changes in both physical and psychological outcomes.
The sample is primarily motor-focused, potentially overlooking non-motor progression.
The cross-sectional design and small sample of 40 participants from limited centers in Isfahan, Iran, limits changes over time and the generalizability of the findings. Additionally, the reliance on subjective self-reports (e.g., Multidimensional Jealousy Scale, Rumination Response Scale) may introduce bias as PD patients may have cognitive or motor impairments.
Future research could use longitudinal designs, larger, more diverse samples, and objective measures (e.g., cortisol levels) in combination with comprehensive assessments.
CONCLUSION
In conclusion, our study demonstrates that general jealousy and rumination are significantly associated with PD stage, with rumination also predicting disease severity. These findings underscore the need for clinicians to attend to both physical and psychological aspects of PD, consistent with a biopsychosocial approach. Our work contributes to understanding this complex disease and supports continued investigation of interventions targeting its non-motor symptoms.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: S.: Contributed to data collection and conducting the study; B.: Contributed to the revision, design, and conducting of the study; R., Z. and S.: Contributed to writing, revision, and submission. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| CBT | = Cognitive Behavioral Therapy |
| HR-QoL | = Health-Related Quality of Life |
| MBSR | = Mindfulness-Based Stress Reduction |
| PD | = Parkinson’s Disease |
| SD | = Standard Deviation |
| SPSS | = Statistical Package for the Social Sciences |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Ethics Committee of the Isfahan Parkinson’s Association, Isfahan, Iran (Approval ID: IPA-1403-021).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
All participants provided written informed consent prior to their involvement in the study. Participants were informed of the study’s purpose, procedures, potential risks, and their right to withdraw at any time without consequence.
AVAILABILITY OF DATA AND MATERIALS
The datasets generated and analyzed during the current study are not publicly available due to ethical restrictions concerning participant confidentiality, as stipulated by the Ethics Committee of the Isfahan Parkinson’s Association. However, anonymized data may be available from the corresponding author upon reasonable request, subject to approval by the ethics committee.
FUNDING
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The study was supported by internal resources from the Isfahan Parkinson’s Association and Al-Zahra Hospital, Isfahan, Iran, which provided access to facilities and participant recruitment support.
ACKNOWLEDGEMENTS
The authors express their gratitude to the participants for their time and willingness to contribute to this research. The authors also thank the staff at Al-Zahra Hospital and the Isfahan Parkinson’s Association for their support in facilitating participant recruitment and providing access to clinical facilities. No external funding was received for these contributions.

